Acropectoral syndrome
| Acropectoral syndrome | |
|---|---|
| Classification and external resources | |
| OMIM | 605967 |
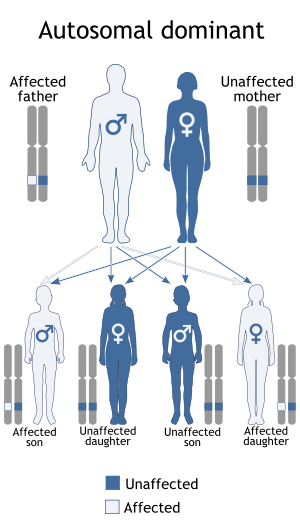
Acropectoral syndrome is an autosomal dominant skeletal dysplasia syndrome affecting the hands, feet, sternum, and lumbosacral spine. A recently proposed candidate gene for preaxial polydactyly is LMBR1, encoding a novel transmembrane receptor, which may be an upstream regulator of SHH.[1] The LMBR1 gene is on human chromosome 7q36.[2]
Summary
Other names for acropectoral syndrome include ACRPS, Syndactyly, preaxial polydactyly and sternal deformity, and ACRP syndrome.[3] This syndrome is characterized by syndactyly of all fingers/toes, pre axial polydactyly in the hands/feet, and upper sternum malformations. More specifically affected individuals show soft tissue syndactyly of all fingers and toes.[4] 14 out of the 22 individuals had pre axial polydactyly, as well had a blind-ending U-shaped sinus in the chest wall or a prominent upper sternum. Other symptoms included an extra big toe and an extra thumb (6). Treatment of individuals affected with this syndrome include oral pathology, facial and limb plastic surgery, and pediatric otolaryngology (7). This syndrome is different than acropectorovertebral dysplasia because the vertebral anomalies seen in acropectorovertebral dysplasia were not observed in these patients. This syndrome also differed from acropectorovertebral dysplasia because of the carpal, tarsal, and metatarsal synostoses as well as the preaxial polydactyly that occurred in the feet as well as in the hands. Soft tissue syndactyly was more prominent that in acropectorovertebral dysplasia.[5] The limb defects seen in acrpectoral syndrome are also similar to those that occur in other dominantly inherited types of preaxial polydactyly, including preaxial polydactyly type II (PPD2), preaxial polydactyly type III (PPD3) and triphalangeal thumb- polysyndactyly (TPT-PS).[1] Acropectoral syndrome is autosomal dominant and best described in 22 patients of a Turkish family spanning six generations. The prevalence of this disease is less than 1 in 1 million.[4]
Mapping
The cytogenetic location is 7q36 and genomic coordinates are GRCh37:147,900,000 - 159,138,663 (NCBI). Mapping of this syndrome was done by Dundar and coworkers in 2001. They showed that this phenotype was linked to a 6.4-cM region of 7q36 flanked by the EN2 gene and the marker D7S2423.[5] Dundar and coworkers characterized and mapped acropectoral syndrome and also showed it was unrelated to acropectorovertebral syndrome. The mapping showed that the acropectoral locus was in a region where preaxial polydactyly and triphalangeal thumb-polysyndactyly had previously been mapped. This study was important because it expanded the range of phenotypes that are connected to this locus. Previously, preaxial polydactyly and sternal defects have been linked to ectopic expression of the gene Sonic hedgehog Shh in limbbud and lateral plate mesoderm during development in mice. Dundar and coworkers found that the LMBR1 gene links to pre axial polydactyly. This gene encodes for a new transmembrane receptor and it is proposed that this receptor is an upstream regulator of SHH.[1]
Clinical features
All 22 individuals studied had partial or complete webbing of the soft tissue between their fingers and toes. In 13 of the individuals the most lateral 3 or 4 toes were flexed at the interphalangeals joints. According to Dundar and coworkers, 8 of the 22 individuals had “pre axial polydactyly in the hands (unilateral in two, bilateral in six), ranging in severity from broad or bifid distal phalanges in the thumbs to duplication of an entire biphalangeal or triphalangeal thumb, in two cases with an associated extra metacarpal, lying in a soft tissue web between the thumb and index finger. Fourteen had preaxial polydactyly in the feet (unilateral in one, bilateral in 13), consisting of a small extra biphalangeal toe, in most cases with an associated rudimentary extra metatarsal, lying in a soft tissue web between the hallux and second toe. In some cases, this was accompanied by hypoplasia of the head of the first metatarsal and absence of both phalanges of the hallux. In addition, 14 had a sternal abnormality, consisting of a pectus carinatum deformity of the upper sternum and/or a pectus excavatum deformity of the lower sternum, producing a blind ending, inverted U shaped sinus in the anterior chest wall. A thoracic CT scan of V.38, who was typically affected, showed an increase in the anterior-posterior diameter of the upper chest, with no underlying bony defect in the sternum. There were no other skeletal or extraskeletal abnormalities”.[1]
Support
Three main support groups of this syndrome are the ASGA in Australia, The Association for Children with Genetic Disorders in Poland, and the Association of People of Genetic Disorders in Greece.[4] For more information: http://rarediseases.info.nih.gov/GARD/Condition/8485/Acropectoral_syndrome.aspx
References
- 1 2 3 4 Dundar M, Gordon TM, Ozyazgan I, et al. (May 2001). "A novel acropectoral syndrome maps to chromosome 7q36". J. Med. Genet. 38 (5): 304–9. doi:10.1136/jmg.38.5.304. PMC 1734869
 . PMID 11333865.
. PMID 11333865. - ↑ Online Mendelian Inheritance in Man (OMIM) 605967
- ↑ "Acropectoral Syndrome". Acropectoral Syndrome. NIH Office of Rare Diseases Research (ORDR). Retrieved 10 Nov 2011.
- 1 2 3 "Orpha Reference". Orphanet. Retrieved 10 Nov 2011.
- 1 2 "OMIM Entry - `5967 - ACROPECTORAL SYNDROME". OMIM - Online Mendelian Inheritance in Man. Retrieved 10 Nov 2011.