Glued IOL
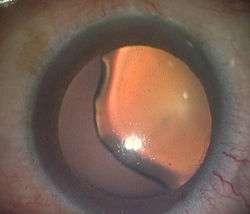
Glued IOL[1] or Glued Intraocular lens is a new Surgical technique for implantation of a posterior chamber IOL with the use of biological glue in eyes with deficient or absent posterior capsules (Fig 1). A quick-acting surgical fibrin sealant derived from human blood plasma,[2][3] with both hemostatic and adhesive properties is used.
Normal Eye
The eye resembles a camera. Just as we take a photograph with the camera, so also the eye takes a photograph of an object seen by it. In the camera, an object is focused onto the film of the camera by a lens. This image is an inverted image and it is developed in the studio and made into an erect one. The same way, an object is focused by the lens of the eye onto the film of the eye called retina. This image is also inverted and is made erect by the brain.
What is Cataract?
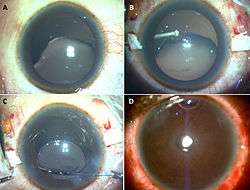
Cataract is an opacity in the lens of the eye. The normal lens allows light to reach the retina. When it becomes opaque and does not allow light to reach the retina, we are unable to see clearly. To understand cataract better, imagine photographing through a camera with grease smeared onto its lens. In such a case, the image formed is very hazy and blurred. Similar to grease smearing onto the lens of a camera, if the lens of the eye gets opaque, the image formed on the retina will be blurred and one will not see clearly. There is no medical treatment for cataract. The only treatment is surgery. When a person has a cataract and the decision is made to operate, then the diseased lens is removed and replaced by an artificial lens called an Intraocular lens or IOL. Once the cataract [diseased lens] is removed, there is no focusing ability of the eye as there is no lens in the eye. So one has to use the IOL to get the object focused onto the retina. For an intraocular lens to be placed in the eye one needs some support which is given by the capsule of the lens which is left behind. But in some cases there is no capsule and in such cases the alternative is to fix a glued IOL (Fig 2). The other alternative is to suture the IOL to the eye or fix it in some other place like an anterior chamber IOL.
Camera Analogy for Glued IOL
To understand why the glued IOL works better compared to a sutured IOL or AC IOL, let us think of a camera. If we break the lens of the camera and fix it back to the camera body with sutures and take photos the picture quality will not be good as the lens would be moving. This is what happens in an eye with a sutured IOL as there is movement of the IOL (pseudo phacodonesis). Imagine if we would glue the lens to the camera body both the lens and the body of the camera would move in unison. This is what happens in a glued IOL and there is no movement of the IOL (pseudo phacodonesis) which gives a better picture quality.
Pioneers
Maggi and Maggi in 1997 were the first to report sutureless scleral fixation of a special IOL. Sutureless intrascleral fixation of posterior chamber IOL was first described by Dr.Gabor Scharioth from Germany.[4][5] This technique was further modified by making scleral flaps and creating scleral pockets for tucking the haptics. The flaps are then reattached to the bed with the help of Glue.
History
On 14 December 2007, at Dr. Agarwal's Eye Hospital, Chennai, India the first glued Intraocular lens (IOL) surgery was done. For the first time in the World, tissue glue had been used to fix an intraocular lens in an eye. This new surgical procedure was invented & performed by Prof. Amar Agarwal, Chairman, Dr.Agarwal’s Eye Hospital, Chennai. Subsequently the first child in whom glued IOL was performed was a patient Anandhi who had a history of injury in her right eye 3 months ago while bursting crackers. She underwent emergency surgery for lens removal due to severe injury to the lens and sutured IOL, which was specific for such cases. After 1 month, when the child came for follow up, it was found that there was a decenteration of IOL. The parents noted the child’s difficulty in performing activities in right eye. Under general anaesthesia Prof. Amar Agarwal removed the already existing IOL and placed the IOL using the Glued IOL technique.
Indication
Glued IOL can be done both as a primary and as a secondary procedure in cases in which the lens capsule is deficient or absent . As a primary procedure it can be done in all cases of intraoperative posterior capsule rupture. It can also be done in all cases of subluxation or dislocation of lens e.g. Marfans syndrome, traumatic dislocation of lens etc. As a secondary procedure it can be done in all the aphakic cases or can also be done as a part of IOL exchange following an anterior chamber IOL, subluxated or dislocated IOL.
Fibrin Glue
Fibrin glue has been used previously in various medical specialties as a hemostatic agent to arrest bleeding, seal tissues and as an adjunct to wound healing. It is available in a sealed pack that contains freeze-dried human fibrinogen (20 mg/0.5 ml), freeze-dried human thrombin (250 IU/0.5 ml), aprotinin solution (1,500 KIU in 0.5 ml), one ampoule of sterile water, four 21-gauge needles, two 20-gauge blunt application needles, and an applicator with two mixing chambers and one plunger guide. Preparation of glue: The vials are placed in a water bath which is preheated to 37 degrees for 2 to 3 minutes. 0.5 cc of distilled water is then added to thrombin vial whereas aprotinin is mixed with fibrinogen. Both the components are then filled in separate syringes and a 26 G needle is attached to it.
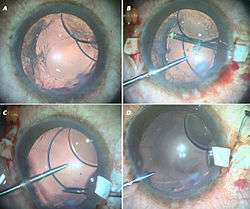
Surgical Technique
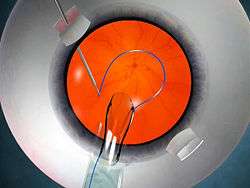
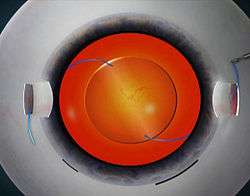
The glued IOL technique consists of making two partial thickness scleral flaps exactly 180° apart approximately 2.5 mm by 2.5 mm followed by a sclerotomy with a 20-gauge needle 1 mm from the limbus. A 23 G vitrectomy cutter is introduced from the sclerotomy site and thorough vitrectomy is done removing all the vitreous tractions. A corneal tunnel is fashioned and then a 23-gauge Glued IOL forceps is passed through the sclerotomy site and the tip of the leading haptic of IOL is grasped, which is then externalised and brought out onto the ocular surface (Fig 3). Similarly the trailing haptic is then externalised using the handshake technique. Scleral pockets are made at the edge of the flap with a 26-gauge needle just parallel to the sclerotomy site, into which the two haptics are then tucked for additional stability (Fig 4). The scleral flaps are then glued back into place using biological glue. The IOLs that can be used are the three-piece foldable IOLs with slightly firm haptics or a three- piece non-foldable IOL. The glue is then used to seal the conjunctival closure.
Vertical Glued IOL
The concept of performing "Vertical glued IOL" was first suggested by Dr. Jeevan Ladi from Pune, India.The vertical corneal diameter is always less than the horizontal diameter. In cases of big eyes, the least corneal diameter (i.e. at 6’o clock & 9’ o clock) along the vertical axis can be chosen for making the scleral flaps. The IOL’s currently available in the market are 13 mm in length. Choosing the least corneal diameter allows extra length of the haptic available for tucking and so gives extra stability.
Advantages: 1. Comfortable temporal seating 2. Vortex veins are not disturbed. So there is less bleeding. 3. The flaps get hidden beneath the lid margin in the fornices. So cosmetically it looks better. 4. Extra length of the haptic is available for tucking. This gives more stability to the IOL.
According to some studies and Dr. Steven Safran[6] it is essential to state that the ciliary sulcus diameter and corneal horizontal white-white diameter may not co-relate totally and it has been suggested that the surgeon can go ahead with horizontal placement of haptics rather than orienting it vertically.
Modifications in Glued IOL Surgery
No-Assistant Technique – This technique works on the principle of vector forces and was performed and discovered by Dr. Priya Narang from Ahmedabad, India.[7][8][9] In this technique, after the externalization of the leading haptic the trailing haptic is flexed beyond the pupillary plane, towards 6’o clock position. This reverses the direction of vector forces and in a way causes the leading haptic to extrude more from the previous sclerotomy site thereby preventing the haptic slippage and its subsequent complications. Plugging Silicon Tires of Iris Hooks - This technique was started by Dr. George Beiko and Dr. Roger Steinert wherein the silicon tires of the iris hooks are plugged on to the leading haptic to prevent its accidental slippage in to the eye.[10] Dr. Steven Safran also started the microbull dog technique for the same purpose. Y-Fixation Technique - This technique was started by Dr. Ohta Toshihiko (Japan) et al. wherein a Y shaped incision is made in the sclera that eliminates the need to make a scleral flap.[11] Mckee Yuri/Francis Price et al. modified the scleral flap making by lifting only two edges of the flap and keeping the flap adherent at the point of haptic enclavation.[12]
Handshake Technique
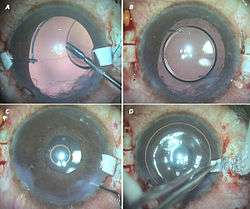
This technique[13] is used for easy externalisation of haptics (Fig 5 and 6) especially for externalisation of the trailing haptic and in cases of small pupil. Two glued IOL forceps are needed for this technique. The haptic is held with one forceps which is introduced from the corneal tunnel and the other forceps is introduced from the sclerotomy site.The tip of the haptic is then traced and is caught followed by externalisation from the sclerotomy site. Visualisation of the tip of the haptic becomes very difficult in cases of small pupil. Although iris hooks can be used the handshake technique simplifies the procedure.The exteriorization of the haptics is a key step in the glued IOL. Since the surgeon is maneuvering with both hands simultaneously, one hand injecting the IOL while the other grasps and exteriorizes the haptics, he/she needs to be familiar with the handshake technique as a means of transferring the haptic from one hand to the other. If one of the haptics is not caught or if it gets released accidentally after grasping it, the situation can be easily resolved using this technique . It utilizes two glued IOL forceps, one of which holds one haptic. Depending on ease of access, the other MST forceps is introduced through the opposite sclerotomy or through the side-port. The first hand then transfers the haptic into the second MST forceps such that the first hand now becomes free. It is essential to hold the haptic at its tip before exteriorizing it so that it doesn't snag on the sclerotomy while being brought out. For this reason, this handshake transfer of the haptic between the two glued IOL forceps is continued till the tip of the haptic is caught by the forceps on the side to which the haptic is to be exteriorized. This technique thus allows easy intra-ocular maneuvering of the entire haptic or IOL within a closed globe system.
Multifocal Glued IOL
Multifocal glued IOLs have been done with the ReZoom (Abbott Medical Optics), and Tecnis (Advanced Medical Optics or AMO) IOLs. This makes it possible to offer the accommodative IOL advantage even to patients with an absent capsule. The modified Prolene polyvinylidene fluoride haptic in these IOLs helps in being more stiff as well as having superior memory. Sutured scleral-fixated IOLs in pediatric eyes have been known to be associated with problems. Multifocal IOLs allow good vision at a range of distances. Monofocal intraocular lenses which are commonly available give clear point of focus in the distance or closer, but you can choose only one focal point. Multifocal intraocular lenses are designed to avoid the need for glasses by providing two or more points of focus. These intraocular lenses are intended to be placed in the capsular bag. Until recently, it was difficult to provide multifocality for patients who had complicated cataract surgeries which lack normal capsules. Aphakia with deficient capsule has been a limitation for obtaining multifocality. Now multifocality is possible even in complicated cataract surgeries by the Multifocal Glued IOL procedure. In this multifocal IOL implantation is done even in eyes with large posterior capsular rupture (PCR) and aphakias with deficient posterior capsule.
Children with Glued IOL
Good results are reported in multiple complicated pediatric glued IOL situations, such as homocystinuria with subluxation, aniridia with cataractous subluxated lens, Weill-Marchesani syndrome with microspherophakia and glaucoma. In dislocated posterior chamber PMMA IOL, the same IOL can be repositioned, thereby reducing the need for further manipulation.
Aniridia Glued IOL

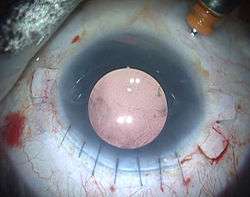
The glued IOL technique can be used in cases in which there is aphakia with aniridia (Fig 7 A and B). In such a cases one can use an aniridia IOL which has got an artificial iris with the IOL component. Thus we can get an aniridia glued IOL.[14]
Glued IOL Scaffold
This procedure combines two techniques i.e. Glued IOL and IOL Scaffold.[15][16] In this technique, glued IOL is performed initially followed by an IOL Scaffold procedure.[17] This technique is specially effective in cases with deficient posterior capsule support and sulcus or iris support. This technique is also applicable for managing traumatic subluxated lens and Soemmering ring.[18]
Pre-Descemet's Endothelial Keratoplasty (PDEK) with Glued IOL
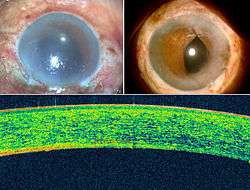
This is a combination of Pre-Descemet's Endothelial Keratoplasty (PDEK)[19] and glued IOL (Fig 8). This combined procedure helps to perform two procedures simultaneously thereby shortening the post-operative visits of the patient to the hospital. Pre Descemet’s endothelial keratoplasty (PDEK) is a kind of endothelial keratoplasty (corneal or eye transplantation), where the pre descemet’s layer (PDL) along with descemet’s membrane (DM) and endothelium is transplanted. The normal cornea has from the front to the back the following layers: 1. Epithelium 2. Bowman's membrane 3. Stroma 4. Pre Descemets layer 5. Descemet's membrane 6. Endothelium
For the human eye to see, the cornea or the front window of the eye should be clear or transparent. For that to happen the inside corneal layer the endothelium pumps out water from the cornea so that the cornea remains transparent and light can pass into the eye and one can see. If the endothelium is bad the cornea starts having lot of water and gets damaged which is called Bullous Keratoplasty. Thus PDEK helps in replacing the non function endothelium in bullous keratopathy. Prof Amar Agarwal (India) in 2013, September 4 performed the first innovative PDEK surgery technique in collaboration with Prof Harminder Dua (UK) and showed the significance of the Pre Descemets layer in corneal transplantation. The initial surgery was performed for pseudophakic bullous keratopathy. Though donor eyes of all age group were used in the initial PDEK cases; there was marked difference in eyes with young donor corneas which resulted in better corneal clarity and visual outcome. This paved the way for the difference of PDEK using young donors and the importance of the endothelial viability. Glued IOL can also be performed with various other corneal transplantation / keratoplasty procedures like Descemet’s memnbrane endothelial keratoplasty (DMEK), Descemet’s stripping endothelail keratoplasty (DSEK) and Penetrating keratoplasty (PK).
Discussion
This glued IOL technique would be useful in many clinical situations in which scleral-fixated IOLs are indicated, such as luxated IOL, dislocated IOL, zonulopathy or secondary IOL implantation. In a case with a dislocated posterior chamber PMMA IOL, the same IOL can be repositioned, thereby reducing the need for further manipulation. Externalization of the greater part of the haptics along the curvature stabilizes the axial positioning of the IOL and thereby prevents any IOL tilt. There is less incidence of uveitis-glaucoma-hyphema syndrome in fibrin glue-assisted IOL implantation as compared with sutured scleral-fixated IOL implantation. In the former, the IOL is well stabilized and stuck onto the scleral bed and thereby has decreased intraocular mobility; in the latter, there is increased possibility of IOL movement or persistent rub over the ciliary body. Visually significant complications due to late subluxation, which has been known to occur in sutured scleral-fixated IOLs, may also be prevented as sutures are avoided in this technique. Moreover, the frequent complications of secondary IOL implantation, such as secondary glaucoma, cystoid macular edema or bullous keratopathy, were not seen in any of our patients. Another important advantage of this technique is the prevention of suture-related complications such as suture erosion, suture knot exposure, or dislocation of IOL after suture disintegration or broken suture. The other advantages of this technique are the rapidity and ease of surgery. The technique eliminates tying the difficult-to-handle 10-0 Prolene suture to the IOL haptic eyelets, the time required to ensure good centration before tying down the knots, and the time required for suturing scleral flaps and closing the conjunctiva, so the total surgical time is significantly reduced. It is also easier and does not require much surgical expertise to use the 25-gauge forceps to grasp and exteriorize the haptic. Fibrin glue takes only 20 seconds to act in the scleral bed, and it helps in adhesion and hemostasis. Fibrin glue has been shown to provide airtight closure, and by the time the fibrin starts degrading, surgical adhesions would have already occurred in the scleral bed.
Summary
Glued IOL implantation is appropriate for eyes with deficient or absent posterior capsule, and this can be performed easily with the available IOL designs and instruments and with less surgical time.
References
- ↑ "Glued intraocular lens: a major review on surgical technique and results". ncbi.nlm.nih.gov//. 2013-01-24. Retrieved 2015-05-22.
- ↑ "Fibrin Glue and Glaucoma Surgery". glaucomatoday.com//. 2008-06-01. Retrieved 2015-05-28.
- ↑ "Antibiotic-Impregnated Fibrin Glue in Ocular Surgery:In vitro Antibacterial Activity". karger.com//. 1999-02-01. Retrieved 2015-05-28.
- ↑ "Sutureless intrascleral posterior chamber intraocular lens fixation". ncbi.nlm.nih.gov//. 2007-11-01. Retrieved 2015-05-29.
- ↑ "Intermediate results of sutureless intrascleral posterior chamber intraocular lens fixation". ncbi.nlm.nih.gov//. 2010-02-01. Retrieved 2015-05-29.
- ↑ "Ciliary sulcus diameter, white-to-white, and the intrascleral haptic fixation technique". ncbi.nlm.nih.gov//. 2015-03-01. Retrieved 2015-05-29.
- ↑ "Modified method of haptic externalization of posterior chamber intraocular lens in fibrin glue-assisted intrascleral fixation: no-assistant technique". ncbi.nlm.nih.gov//. 2013-01-01. Retrieved 2015-05-29.
- ↑ "Postoperative analysis of glued intrascleral fixation of intraocular lens and comparison of intraoperative parameters and visual outcome with 2 methods of haptic externalization". ncbi.nlm.nih.gov//. 2013-06-01. Retrieved 2015-05-29.
- ↑ "Glue-assisted intrascleral fixation of posterior chamber intraocular lens". ncbi.nlm.nih.gov//. 2013-04-01. Retrieved 2015-05-29.
- ↑ "Modification of externalized haptic support of glued intraocular lens technique". ncbi.nlm.nih.gov//. 2013-03-01. Retrieved 2015-05-29.
- ↑ "Simplified and safe method of sutureless intrascleral posterior chamber intraocular lens fixation: Y-fixation technique". ncbi.nlm.nih.gov//. 2014-01-01. Retrieved 2015-05-29.
- ↑ "Implementation of the posterior chamber intraocular lens intrascleral haptic fixation technique (glued intraocular lens) in a United States practice: Outcomes and insights". ncbi.nlm.nih.gov//. 2014-12-01. Retrieved 2015-05-29.
- ↑ "Handshake technique for glued intrascleral haptic fixation of a posterior chamber intraocular lens". ncbi.nlm.nih.gov//. 2013-03-01. Retrieved 2015-05-29.
- ↑ "Combined surgical management of capsular and iris deficiency with glued intraocular lens technique". ncbi.nlm.nih.gov//. 2013-05-29. Retrieved 2015-05-29.
- ↑ "Glued intraocular lens scaffolding to create an artificial posterior capsule for nucleus removal in eyes with posterior capsule tear and insufficient iris and sulcus support". jcrsjournal.org//. 2012-10-04. Retrieved 2015-05-29.
- ↑ "Clinical outcomes of intraocular lens scaffold surgery: a one-year study". ncbi.nlm.nih.gov//. 2013-06-28. Retrieved 2015-05-29.
- ↑ "Glued intraocular lens scaffolding to create an artificial posterior capsule for nucleus removal in eyes with posterior capsule tear and insufficient iris and sulcus support". ncbi.nlm.nih.gov//. 2013-03-01. Retrieved 2015-05-29.
- ↑ "Glued intraocular lens scaffolding for Soemmerring ring removal in aphakia with posterior capsule defect". ncbi.nlm.nih.gov//. 2015-04-01. Retrieved 2015-05-29.
- ↑ "Pre-Descemet's endothelial keratoplasty (PDEK)". ncbi.nlm.nih.gov//. 2014-03-21. Retrieved 2015-05-21.