John F. Kennedy autopsy
The autopsy of President John F. Kennedy was performed, beginning at about 8 p.m. EST November 22, 1963, on the day of his assassination and ending at about 12:30 AM EST November 23, 1963, at the Bethesda Naval Hospital in Bethesda, Maryland. The choice of autopsy hospital in the Washington, D.C. area was made by the now former President's widow, Jacqueline Kennedy. She chose the Bethesda Naval Hospital because President Kennedy had been a naval officer.[1]
Background
On November 22, 1963, Dallas County medical examiner Earl Rose was in his office at Parkland Memorial Hospital across the corridor from Trauma Room 1 when he received word that President Kennedy was pronounced dead.[2] He walked across the corridor to the trauma room occupied by Jacqueline Kennedy and a priest who had been called in to administer last rites.[2] There, Rose was met by Secret Service agent Roy Kellerman and Kennedy's personal physician George Burkley who told him that there was no time for an autopsy because Mrs. Kennedy would not leave Dallas without her husband's body which was to be delivered promptly to the airport.[2] At the time of the assassination of Kennedy, the murder of a United States President was not covered by federal law.[3] Rose objected, insisting that Texas law required him to perform a post-mortem examination prior to the removal of the body.[2][3] A heated exchange ensued as he argued with Kennedy's aides.[2][3] Kennedy's body was placed in a casket and, accompanied by Mrs. Kennedy, rolled down the corridor on a gurney.[2] Rose was reported to have stood in a hospital doorway, backed by a policeman, in an attempt to prevent the removal of the coffin.[2][3] According to Robert Caro's The Years of Lyndon Johnson: The Passage of Power the President's aides "had literally shoved [Rose] and the policeman aside to get out of the building."[2] In an interview with Journal of the American Medical Association, Rose stated that he stepped aside feeling that it was unwise to exacerbate the tension.[2]
Death certificates
Kennedy's personal physician, Rear Admiral George Gregory Burkley, signed a death certificate on November 23 and noted the cause of death as "Gunshot wound, skull".[4][5] Buckley described the head wound as "shattering in type causing a fragmentation of the skull and evulsion of three particles of the skull at time of the impact, with resulting maceration of the right hemisphere of the brain.[5] He also noted "a second wound occurred in the posterior back at about the level of the third thoracic vertebra".[5] A second certificate of death, signed on December 6 by Theron Ward, a Justice of the Peace in Dallas County, stated that Kennedy "came to his death as a result of two gunshot wounds (1) near the center of the body and just above the right shoulder, and (2) 1 inch to the right center of the back of the head."[6]
Official findings of the autopsy
The gunshot wound in the back
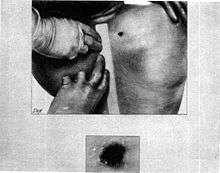
- The Bethesda autopsy physicians attempted to probe the bullet hole in the base of Kennedy's neck above the scapula, but were unsuccessful as it passed through neck strap muscle. They did not perform a full dissection or persist in tracking, as throughout the autopsy, they were unaware of the exit wound, at the front of the throat. Emergency room physicians had obscured it when they performed the tracheotomy.
- At Bethesda, the autopsy report of the president, Warren Exhibit CE 387[7] described the back wound as being oval, 6 by 4 millimetres (0.24 in × 0.16 in), and located "above the upper border of the scapula" (shoulder blade) at a location 14 centimetres (5.5 in) from the tip of the right acromion process, and 14 centimetres (5.5 in) below the right mastoid process (the bony prominence behind the ear).
- The concluding page of the Bethesda autopsy report,[7] states: "The other missile [the bullet to the back] entered the right superior posterior thorax above the scapula, and traversed the soft tissues of the supra-scapular and the supra-clavicular portions of the base of the right side of the neck."
- The report also reported contusion (bruise) of the apex (top tip) of the right lung in the region where it rises above the clavicle, and noted that although the apex of the right lung and the parietal pleural membrane over it had been bruised, they were not penetrated, indicating passage of a missile close to them, but above them.
The report noted that the thoracic cavity was not penetrated. - This missile produced contusions of the right apical parietal pleura and of the apical portion of the right upper lobe of the lung. The missile contused the strap muscles of the right side of the neck, damaged the trachea, and made its exit through the anterior surface of the neck.
- The single bullet of the Warren Commission Report places a bullet wound at the sixth cervical vertebra (C6) of the vertebral column, which is consistent with 5.5 inches (14 cm) below the ear. The Warren Report itself does not conclude bullet entry at the sixth cervical vertebra, but this conclusion was made in a 1979 report on the Kennedy assassination by the HSCA, which noted a defect in the C6 vertebra in the Bethesda X-rays, which the Bethesda autopsy physicians had missed, and did not note. The X-rays were taken by Commander John H. Ebersole, Medical Corps, US Navy.
Even without this information, the original Bethesda autopsy report, included in the Warren Commission report, concluded that this bullet had passed entirely through the president's neck, from a level over the top of the scapula and lung (and the parietal pleura over the top of the lung), and through the lower throat.
The gunshot wound to the head
| GRAPHIC WARNING: a color picture of President Kennedy's head wound taken at the beginning of the autopsy |
|---|
 A picture of President Kennedy's head taken at the beginning of the autopsy |
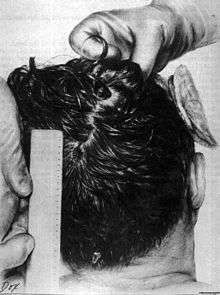
- The wound to the back of the head is described by the Bethesda autopsy as being a laceration measuring 15 by 6 millimetres (0.59 in × 0.24 in), situated to the right and slightly above the external occipital protuberance. In the underlying bone is a corresponding wound through the skull showing beveling (a cone-shaped widening) of the margins of the bone when viewed from the interior of the skull.[8]
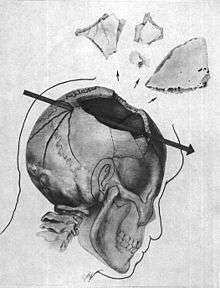
- The large, irregularly shaped defect in the right side of the head (chiefly to the parietal bone, but also involving the temporal and occipital bone) is described as being about 13 centimetres (5.1 in) wide at the largest diameter.[8]
- Three fragments of skull bone were received as separate specimens, roughly corresponding to the dimensions of the large defect. In the largest of the fragments is a portion of the perimeter of a roughly circular wound presumably of exit, exhibiting beveling of the exterior of the bone, and measuring about 2.5 to 3.0 centimetres (0.98 to 1.18 in). X-rays revealed minute particles of metal in the bone at this margin.[8]
- Minute fragments of the projectile were found by X-ray along a path from the rear wound to the parietal area defect.[9]
Later government investigations
Ramsey Clark Panel Analysis (1968)
At the request of the Attorney General of the United States Ramsey Clark, four physicians (hereafter sometimes referred to as The Panel) met in Washington, DC on February 26 and 27 to examine various photographs, X-ray films documents and other evidence pertaining to the death of President Kennedy, and to evaluate their significance in relation to the medical conclusions recorded in the Autopsy Report on the body of President Kennedy signed by Commander J. J. Humes, Medical Corps, US Navy; Commander J. Thornton Boswell, Medical Corps, US Navy and Lt. Col. Pierre A. Finck, Medical Corps, US Army and in the Supplemental Report signed by Commander Humes. These appear in the Warren Commission Report at pages 538 to 545.
The Clark panel reviewed the original autopsy records, photos, and X-rays, as well as clothing, films, motion pictures, and bullet fragments. They also reviewed the Warren Commission report. The Clark panel concluded the following:
Major findings regarding the two missile wounds:
Skull: There are multiple fractures of the bones of the calvarium bilaterally. These fractures extend into the base of the skull and involve the floor of the anterior fossa on the right side as well as the middle fossa in the midline. With respect to the right frontoparietal[10] region of the skull, the traumatic damage is particularly severe with extensive fragmentation of the bony structures from the midline of the frontal bone anteriorly to the vicinity of the posterior margin of the parietal bone behind. Above the fragmentation extends approximately 25 mm. across the midline to involve adjacent portions of the left parietal bone; below, the changes extend into the right temporal bone. Throughout this region, many of the bony pieces have been displaced outward; several pieces are missing. Distributed through the right cerebral hemisphere are numerous small, irregular metallic fragments most of which are less than 1 mm. in maximum dimension. The majority of these fragments lie anteriorly and superiorly. None can be visualized on the left side of the brain and none below a horizontal plane through the floor of the anterior fossa of the skull. On one of the lateral films of the skull (#2), a hole measuring approximately 8 mm. in diameter on the outer surface of the skull and as much as 20 mm. on the internal surface can be seen in profile approximately 100 mm. above the external occipital protuberance. The bone of the lower edge of the hole is depressed. Also there is, embedded in the outer table of the skull close to the lower edge of the hole, a large metallic fragment which on the anteroposterior film (#1) lies 25 mm. to the right of the midline. This fragment as seen in the latter film is round and measures 6.5 mm in diameter immediately adjacent to the hole on the internal surface of the skull, there is localized elevation of the soft tissues. Small fragments of bone lie within portions of these tissues and within the hole itself. These changes are consistent with an entrance wound of the skull produced by a bullet similar to that of exhibit CE 399. The metallic fragments visualized within the right cerebral hemisphere fall into two groups. One group consists of relatively large fragments, more or less randomly distributed. The second group consists of finely divided fragments, distributed in a posteroanterior direction in a region 45 mm. long and 8 mm. wide. As seen on lateral film #2, this formation overlies the position of the coronal suture; its long axis, if extended posteriorly, passes through the above-mentioned hole. It appears to end anteriorly immediately below the badly fragmented frontal and parietal bones just anterior to the region of the coronal suture. The foregoing observations indicate that the decedent's head was struck from behind by a single projectile. It entered the occipital region 25 mm to the right of the midline and 100 mm. above the external occipital protuberance. The projectile fragmented on entering the skull, one major section leaving a trail of fine metallic debris as it passed forward and laterally to explosively fracture the right frontal and parietal bones as it emerged from the head. In addition to the foregoing, it is noteworthy that there is no evidence of projectile fragments in the left cerebral tissues or in the right cerebral hemisphere below a horizontal plane passing through the floor of the anterior fossa of the skull. Also, although the fractures of the calvarium extend to the left of the midline and into the anterior and middle fossa of the skull, no bony defect, such as one created by a projectile either entering or leaving the head, is seen in the calvarium to the left of the midline or in the base of the skull. Hence, it is not reasonable to postulate that a projectile passed through the head in a direction other than that described above. Of further note, when the X-ray films of the skull were presented to The Panel, film #1 had been damaged in two small regions by what appears to be the heat from a spotlight. Also, on film #2, a pair of converging pencil lines had been drawn on the film. Neither of these artifacts interfered with the interpretation of the films.
Neck Region: Films #8, 9, and 10 allowed visualization of the lower neck. Subcutaneous emphysema is present just to the right of the cervical spine immediately above the apex of the right lung. Also, several, small metallic fragments are present in this region. There is no evidence of fracture of either scapula or of the clavicles, or of the ribs or of any of the cervical and thoracic vertebrae. The foregoing observations indicate that the pathway of the projectile involving the neck was confined to a region to the right of [t]he spine and superior to a plane passing through the upper margin of the right scapula, the apex of the right lung and the right clavicle. Any other pathway would have almost certainly fractured one or more bones of the right shoulder girdle and thorax.
DISCUSSION: The information disclosed by the joint examination of the foregoing exhibits by the members of The Panel supports the following conclusions; The decedent was wounded by two bullets, both of which entered his body from behind. One bullet struck the back of the decedent's head well above the external occipital protuberance. Based upon the observation that he was leaning forward with his head turned obliquely to the left when this bullet struck, the photographs and X-rays indicate that it came from a site above and slightly to his right. This bullet fragmented after entering the cranium, one major piece of it passing forward and laterally to produce an explosive fracture of the right side of the skull as it emerged from the head. The absence of metallic fragments in the left cerebral hemisphere or below the level of the frontal fossa on the right side together with the absence of any holes in it the skull to the left of the midline or in its base and the absence of any penetrating injury of the left hemisphere, eliminate with reasonable certainty the possibility of a projectile having passed through the head in any direction other than from back to front as described in preceding sections of this report. The other bullet struck the decedent's back at the right side of the base of the neck between the shoulder and spine and emerged from the front of his neck near the midline. The possibility that this bullet might have followed a pathway other than one passing through the site of the tracheotomy wound was considered. No evidence for this was found. There is a track between the two cutaneous wounds as indicated by subcutaneous emphysema and small metallic fragments on the X-rays and the contusion of the apex of the right lung and laceration of the trachea described in the Autopsy Report. In addition, any path other than one between the two cutaneous wounds would almost surely have been intercepted by bone and the X-ray films show no bony damage in the thorax or neck. The possibility that the path of the bullet through the neck might have been more satisfactorily explored by the insertion of a finger or probe was considered. Obviously the cutaneous wound in the back was too small to permit the insertion of a finger. The insertion of a metal probe would have carried the risk of creating a false passage in part, because of the changed relationship of muscles at the time of autopsy and in part because of the existence of postmortem rigidity. Although the precise path of the bullet could undoubtedly have been demonstrated by complete dissection of the soft tissue between the two cutaneous wounds, there is no reason to believe that the information disclosed thereby would alter significantly the conclusions expressed in this report.
SUMMARY: Examination of the clothing and of the photographs and X- rays taken at autopsy reveal that President Kennedy was struck by two bullets fired from above and behind him, one of which traversed the base of the neck on the right side without striking bone and the other of which entered the skull from behind and exploded its right side. The photographs and X-rays discussed herein support the above-quoted portions of the original Autopsy Report and the above-quoted medical conclusions of the Warren Commission Report.[11]
Major differences with, and support of, conclusions in the Bethesda autopsy and Warren Report:
- The Clark report places the head bullet wound 100 mm (4 inches) above the reported occipital protuberance wound of the Bethesda report. This is important, because it is consistent with a high angle rear entry wound to the skull.
- The Clark report places the back wound squarely in the neck above the scapula and passing through the throat, passing over the TOP of the right lung, in keeping with the Bethesda conclusions. However, this finding is bolstered by additional findings of metallic fragments along the higher bullet trail.
Rockefeller Commission analysis (1975)
The five-member Rockefeller Commission, which included three pathologists, a radiologist, and a wound ballistics expert, did not address the back and throat wounds, writing in its report, "The investigation was limited to determining whether there was any credible evidence pointing to CIA involvement in the assassination of President Kennedy," and that "The witnesses who presented evidence believed sufficient to implicate the CIA in the assassination of President Kennedy placed much stress upon the movements of the President's body associated with the head wound that killed the President."
The Commission examined the Zapruder, Muchmore, and Nix films, the 1963 autopsy report, the autopsy photographs and X-rays, President Kennedy's clothing and back brace, the bullet and bullet fragments recovered, the 1968 Clark Panel report, and other materials. The five panel members came to the unanimous conclusion that President Kennedy was struck by only two bullets, both of which were fired from the rear, including one that struck the back of the head. Three of the physicians reported that the backward and leftward motion of the President's upper body following the head shot was caused by a "violent straightening and stiffening of the entire body as a result of a seizure-like neuromuscular reaction to major damage inflicted to nerve centers in the brain."
The report added that there was "no evidence to support the claim that President Kennedy was struck by a bullet fired from either the grassy knoll or any other position to his front, right front or right side … No witness who urged the view [before the Rockefeller Commission] that the Zapruder film and other motion picture films proved that President Kennedy was struck by a bullet fired from his right front was shown to possess any professional or other special qualifications on the subject."[12]
HSCA analysis (1979)

The United States House Select Committee on Assassinations (HSCA) contained a forensic panel which undertook the unique task of reviewing original autopsy photographs and X-rays and interviewed autopsy personnel, as to their authenticity. The Panel and HSCA then went on to make medical conclusions based on this evidence.
The HSCA's major medical-forensic conclusion was that "President Kennedy was Struck by Two Rifle Shots Fired from Behind Him;"[13] The committee found acoustic evidence of a second shooter, but concluded that this shooter did not contribute to the president's wounds, and therefore was irrelevant to the autopsy results.
The committee's forensic pathology panel was composed of nine members, eight of whom were chief medical examiners in major local jurisdictions in the United States. As a group, they had been responsible for more than 100,000 autopsies, an accumulation of experience the committee deemed invaluable in the medical evidence evaluation — including the autopsy X-rays and photographs — to determine the cause of the President's death and the nature and location of his wounds.
The committee also employed experts to authenticate the autopsy materials. Neither the Clark Panel nor the Rockefeller Commission undertook to determine if the X-rays and photographs were, in fact, authentic. The committee, in light of the numerous issues that had arisen over the years with respect to autopsy X-rays and photographs, believed authentication to be a crucial step in the investigation. The authentication of the autopsy X-rays and photographs was accomplished by the committee with the assistance of its photographic evidence panel as well as forensic dentists, forensic anthropologists, and radiologists working for the committee. Two questions were put to these experts:
1. Could the photographs and X-rays stored in the National Archives be positively identified as being of President Kennedy?
2. Was there any evidence that any of these photographs or X-rays had been altered in any manner?
To determine if the photographs of the autopsy subject were in fact of the President, forensic anthropologists compared the autopsy photographs with ante-mortem pictures of him. This comparison was done on the basis of both metric and morphological features. The metric analysis relied upon various facial measurements taken from the photographs, while the morphological analysis was focused on consistency of physical features, particularly those that could be considered distinctive, such as the shape of the nose, patterns of facial lines, e.t. Once unique characteristics were identified, posterior and anterior autopsy photographs were compared to verify that they depicted the same person.
The anthropologists studied the autopsy X-rays in conjunction with premortem X-rays of the President. A sufficient number of unique anatomic characteristics were present in X-rays taken before and after the President's death to conclude that the autopsy X-rays were of President Kennedy. This conclusion was consistent with the findings of a forensic dentist employed by the committee. Since many of the X-rays taken during the course of the autopsy included the Kennedy's teeth, it was possible to determine, using the his dental records, that the X-rays were of the President.
Once the forensic dentist and anthropologists had determined that the autopsy photographs and X-rays were of the President, photographic scientists and radiologists examined the original autopsy photographs, negatives, transparencies, and X-rays for signs of alteration. They concluded there was no evidence of the photographic or radiographic materials having been altered. Consequently, the committee determined that the autopsy X-rays and photographs were a valid basis for the conclusions of the committee's forensic pathology panel.
While the examination of the autopsy X-rays and photographs was the principal basis of its analysis, the forensic pathology panel also had access to all relevant witness testimony. In addition, all tests and evidence analyses requested by the panel were performed. It was only after considering all of this evidence that the panel reached its conclusions.
The pathology panel concluded that President Kennedy was struck by only two bullets, each of which entered from the rear. The panel further concluded that the President was struck by "one bullet that entered in the upper right of the back and exited from the front of the throat, and one bullet that entered in the right rear of the head near the cowlick area and exited from the right side of the head, toward the front" saying that "this second bullet caused a massive wound to the President's head upon exit." The panel concluded that there was no medical evidence that the President was struck by a bullet entering the front of the head and the possibility that a bullet could have struck him, and yet left no evidence has been extremely remote.
Because this conclusion appeared to be inconsistent with the backward motion of the President's head in the Zapruder film, the committee consulted a wound ballistics expert to determine what relationship, if any, exists between the direction from which a bullet strikes the head and subsequent head movement. The expert concluded that nerve damage from a bullet entering the President's head could have caused his back muscles to tighten which, in turn, could have forced his head to move toward the rear. He demonstrated the phenomenon in a filmed experiment which involved the shooting of goats. Thus, the committee determined that the rearward movement of the President's head would not be fundamentally inconsistent with a bullet striking from the rear.[14]
The HSCA also voiced certain criticisms of the original Bethesda autopsy and handling of evidence from it. These included:
- the "entrance head wound location was incorrectly described.”
- The autopsy report was “incomplete”, prepared without reference to the photographs, and was “inaccurate” in a number of areas, including the entry in Kennedy's back.
- The ”entrance and exit wounds on the back and front neck were not localized with reference to fixed body landmarks and to each other”.
Document inventory analysis: Assassination Records Review Board (1992–98)
The Assassination Records Review Board (ARRB) was created by the President John F. Kennedy Assassination Records Collection Act of 1992, which mandated the gathering and opening of all US government records related to the assassination.[15] The ARRB began work in 1994 and produced a final report four years later.[16] The Board partially credited public concern about conclusions in the 1991 Oliver Stone movie JFK for passage of the legislation that created the ARRB. The Board noted that the movie "popularized a version of President Kennedy’s assassination that featured U.S. government agents from the Federal Bureau of Investigation (FBI), the Central Intelligence Agency (CIA), and the military as conspirators."[17]
According to Douglas P. Horne, the ARRB's chief analyst for military records,
The Review Board’s charter was simply to locate and declassify assassination records, and to ensure they were placed in the new “JFK Records Collection” in the National Archives, where they would be freely available to the public. Although Congress did not want the ARRB to reinvestigate the assassination of President Kennedy, or to draw conclusions about the assassination, the staff did hope to make a contribution to future ‘clarification’ of the medical evidence in the assassination by conducting these neutral, non-adversarial, fact-finding depositions. All of our deposition transcripts, as well as our written reports of numerous interviews we conducted with medical witnesses, are now a part of that same collection of records open to the public. Because of the Review Board’s strictly neutral role in this process, all of these materials were placed in the JFK Collection without comment.[18]
The ARRB sought additional witnesses in an attempt to compile a more complete record of the autopsy on Kennedy.[19] In July 1998, a staff report released by the ARRB emphasized shortcomings in the original autopsy.[19] The ARRB wrote, "One of the many tragedies of the assassination of President Kennedy has been the incompleteness of the autopsy record and the suspicion caused by the shroud of secrecy that has surrounded the records that do exist."[19]
Personnel present during autopsy
List of personnel present at various times during the autopsy, with official function, taken from the Sibert-O'Neill report list, the HSCA list[20] and attorney Vincent Bugliosi, author of Reclaiming History: The Assassination of President John F. Kennedy.
Non-medical personnel from law-enforcement/security:
- John J. O'Leary: Secret Service agent.
- William Greer: Secret Service agent.
- Roy Kellerman: Secret Service agent.
- Francis X. O'Neill: FBI special agent
- James "Jim" Sibert: FBI special agent, assisting Francis O'Neill[21]
Medical personnel and assistants (USA = US Army, USN = US Navy, USAF = US Air Force, MC = Medical Corps)
Official autopsy signatories:
- Commander J. Thornton Boswell, MC, USN: chief of pathology at Naval Medical Center, Bethesda.
- Commander James J. Humes, MC, USN: director of laboratories of the National Medical School, Naval Medical Center, Bethesda. Chief autopsy pathologist for the JFK autopsy. Officially conducted autopsy.
- Lieutenant Colonel Pierre A. Finck, MC, USA: Chief of the military environmental pathology division and chief of the wound ballistics pathology branch at Walter Reed Medical Center.
Other medical personnel
- John Thomas Stringer, Jr: medical photographer
- Floyd Albert Riebe: medical photographer
- PO Raymond Oswald, USN: medical photographer on call
- Paul Kelly O'Connor: laboratory technologist
- James Curtis Jenkins: laboratory technologist
- Edward F. Reed: X-ray technician
- Jerrol F. Custer: X-ray technician
- Jan Gail Rudnicki: Dr. Boswell's lab tech assistant on the night of the autopsy
- PO James E. Metzler, USN: Hospital Corpsman 3rd Class
- James H. Ebersole: Assistant Chief of Radiology
- Lieutenant Commander Gregory H. Cross, MC, USN: resident in surgery
- CPO Chester H. Boyers, USN: chief petty officer in charge of the pathology division, visited the autopsy room during the final stages to type receipts given by FBI and Secret Service for items obtained
- Vice Admiral Edward C. Kenney, MC, USN: surgeon general of the U.S. Navy
- Dr. George Bakeman, USN
- Rear Admiral George Burkley, M.D., MC, USN: the president’s personal physician
- Captain James M. Young, M.D., MC, USN: the attending physician to the White House
- Robert Frederick Karnei, M.D.: Bethesda pathologist
- Captain David P. Osborne, MC, USN: chief of surgery at Bethesda
- Captain Robert O. Canada, USN: commanding officer of Bethesda Naval Hospital
Additional military personnel
- Brigadier General Godfrey McHugh, USAF: US military aide to the President on the Dallas trip
- Rear Admiral Calvin B. Galloway, USN: commanding officer of the U.S. Naval Medical Center, Bethesda
- Captain John H. Stover, Jr., USN: commanding officer of the U.S. Naval Medical School, Bethesda
- Major General Philip C. Wehle, USA: commanding officer of the U.S. Military District of Washington, D.C., entered to make arrangements for the funeral and lying in state.
- 2nd Lieutenant Richard A. Lipsey, USA: Jr. aide to General Wehle[22]
- 1st Lieutenant Samuel A. Bird, USA: head of the Old Guard.
- Sr CPO, Alexander Wadas - Chief on duty.
Others: At the termination of the autopsy, the following personnel from Gawler’s Funeral Home entered the autopsy room to prepare the President’s body for viewing and burial (this required 3 to 4 hours ):
- John VanHoesen
- Edwin Stroble
- Thomas E. Robinson
- Joe Hagen
References
![]() Media related to Photos of the autopsy of John F. Kennedy at Wikimedia Commons
Media related to Photos of the autopsy of John F. Kennedy at Wikimedia Commons
- ↑ President John F Kennedy Assassination Report of the Warren Commission. 2004. p. 43. ISBN 0-974-77691-2.
- 1 2 3 4 5 6 7 8 9 Stafford, Ned (July 13, 2012). "Earl Rose: Pathologist prevented from performing autopsy on US President John F Kennedy" (PDF). BMJ. 345. doi:10.1136/bmj.e4768. Retrieved November 3, 2014.
- 1 2 3 4 Munson, Kyle (April 28, 2012). "Munson: Iowan more than a footnote in JFK lore". The Des Moines Register. Indianapolis. Retrieved November 3, 2014.
- ↑ WGBH Educational Foundation. "Oswald's Ghost". American Experience. PBS. Retrieved January 5, 2014.
- 1 2 3 Burkley, George Gregory (November 23, 1963). "Certificate of Death". National Archives and Records Administration. front side, back side. NAVMED Form N – via The President John F. Kennedy Assassination Records Collection.
- ↑ "Part IV". Appendix to Hearings before the Select Committee on Assassinations of the U.S. House of Representatives. VII. Washington, D.C.: United States Government Printing Office. March 1979. p. 190.
- 1 2 Commission Exhibit 387
- 1 2 3 Appendix IX: Autopsy Report and Supplemental Report, Warren Commission Report, p. 541.
- ↑ Appendix IX: Autopsy Report and Supplemental Report, Warren Commission Report, p. 543.
- ↑ That is, involving both the frontal and parietal bones.
- ↑ "Clark Panel On the Medical Evidence". Jfklancer.com. Retrieved 2013-02-07.
- ↑ Allegations That President Kennedy Was Struck in the Head by a Bullet Fired From His Right Front, Chapter 19: Allegations Concerning the Assassination of President Kennedy, Rockfeller Commission Report.
- ↑ "Findings". Archives.gov. Retrieved 2013-02-07.
- ↑ "Findings". Archives.gov. Retrieved 2013-02-07.
- ↑ Assassination Records Review Board (September 30, 1998). "Executive Summary". Final Report of the Assassination Records Review Board (pdf). Washington, D.C.: United States Government Printing Office. p. xxiii. Retrieved June 10, 2015.
- ↑ Final Report of the Assassination Records Review Board, Chapter 1 1998, p. 6.
- ↑ Final Report of the Assassination Records Review Board, Chapter 1 1998, p. 1.
- ↑ Prepared Remarks by Douglas P. Horne, Former Chief Analyst for Military Records, Assassination Records Review Board (ARRB), Press Conference at the Willard Hotel, Washington, D.C., May 15, 2006.
- 1 2 3 Lardner Jr., George (August 2, 1998). "Gaps in Kennedy Autopsy Files Detailed". The Washington Post. Retrieved July 22, 2015.
- ↑ Section II - Performance of Autopsy
- ↑ Miller, Glenn (November 22, 2009). "Ex-FBI agent who watched JFK autopsy reflects on death". USA Today. Retrieved March 13, 2013.
- ↑ "HSCA INTERVIEW WITH RICHARD LIPSEY, 1-18-78". History-matters.com. 1939-10-07. Retrieved 2013-02-07.
{kind=link}
{kind=link}
Primary sources
- Sibert/O'Neill FBI autopsy report original.
- A second cached version at Archive.is (archived 2012-12-15). This primary document preserves the notes of two FBI agents (Special Agents James W. Sibert and Francis X. O'Neill) who were present at the autopsy and took notes. It is helpful on times and personnel, but the agents were non-medically trained people who did not completely understand what they were seeing in the actual autopsy wounds. Moreover, the early report preserves genuine medical doctor confusion present actually during the autopsy, caused by apparent lack of an exit wound, which was cleared up later in the official report after new and more complete information became available. However, as a primary piece of observation by medical laymen, the report is useful.
- Official autopsy written report, taken from the Warren Commission report, CE (Commission Exhibit) 387.
Secondary sources
| Wikimedia Commons has media related to Photos of the autopsy of John F. Kennedy. |
- Joe Backes, The State of the Medical Evidence in the JFK Assassination; Doug Horne's presentation at JFK Lancer 1998 Conference.
- JFK Assassination Medical Evidence.