Pre-hospital trauma assessment
Pre-hospital trauma assessment is a set of skills used by emergency medical services technicians to analyze all threats to life that a patient could suffer due to a trauma incident. Pre-hospital trauma assessment is broken into two major types: basic trauma assessment and advanced trauma assessment. The basic assessment is provided by first responders and EMTs. The advanced assessment is provided by a paramedic.
Steps
- Scene size-up
- Initial assessment
- Focused history and physical examination
- Detailed physical examination
- Ongoing assessment
- Communications
- Documentation
Scene size-up
Approaching and sizing up a trauma incident scene is one of the most important primary steps that a pre-hospital care provider carefully does. Within a critical trauma incident, seeing hazardous material and traffic in an uncontrolled environment is expected. These factors can cause life-threats for providers, coworkers, and bystanders. Therefore, controlling all these life-threats is initially accomplished even before patient contact.
After scene management, a pre-hospital care provider gets a general impression of the scene. A general impression is discovered by evaluating the mechanism of injury. For example, in a car accident, mechanism of injury is detected by estimating the speed at which the collision occurred, looking at the amount of damage, and looking for other factors that may affect the mechanism of injury, such as airbag deployment.
This general impression helps the provider to make some important decisions regarding the number and type of transport units needed, and also helps to determine how critical a patient is.
Scene size-up consists of several steps which may be performed in different orders dependent upon circumstance:
- Body substance isolation precautions
- Scene safety
- Mechanism of injury
- Number of patients and need for additional help
- Consider c-spine immobilization
Critical to the scene size-up is the need for quick decisions to be made. In the absence of hazards delaying progress, such decisions should be made by the time the patient is reached.
Initial assessment
The initial assessment for trauma patients does not differ from medical patient assessment. The primary outcome of the initial assessment is to determine any "immediate life threats".
The first step in performing an initial assessment is forming a general impression - is this patient "sick", "not sick", or "not sure". Taking steps to immobilize the patient's head to prevent any or any further injury to the spine, the level of consciousness is assessed according to the AVPU criteria - Alert, responds to Verbal stimuli, responds to Pain stimuli, Unresponsive.
After checking the level of responsiveness, ABC is checked. ABC stands for airway, breathing, and circulation. In a trauma patient, sometimes the airway gets blocked due to facial injury or foreign body objects. According to Sanders, a patent airway should be maintained by positioning the patient properly, removing all blocking objects and carefully positioning the head using jaw-thrust technique.
The next step after maintaining a patent airway is checking breathing rate and quality. If the patient is breathing less than 8 times/minute or shallow more than 35/minutes, the patient then needs somebody to breathe for him using a [bag valve mask] attached to a high flow oxygen source.
Then, checking the pulse comes as the third step. For responsive adult patients, a pulse assessment is usually done by palpating the radial artery, which is located on the inside of the wrist toward the thumb. For unresponsive adult patients, checking pulse is performed by palpating the carotid artery in the neck. For infants and small children, the pulse is usually assessed in the brachial artery in the upper arm. After confirming that the pulse is present, the final step in the initial assessment for a trauma patient is to check for any gross bleeding and to control it. Should a pulse not be detected, or in the case of a child or infant is present but at a rate less than 60, cardiovascular resuscitation will be commenced.
Steps:
- General impression of the patient
- Assessing the patient's mental status
- Assessing the patient's airway status
- Assessing the patient's breathing status
- Assessing the patient's circulation
- Identifying priority patients
Focused history and physical examination
In a critical trauma incident, more than one provider is needed to be available to perform an assessment on one patient. After the initial assessment, one of the providers checks vital signs and looks for any information about the patient's medical history. Other providers work on physically examining the patient to look for any life threats or other problems that can be fixed while en route to the hospital. A rapid head-to-toe exam is performed to look for any deformities, contusions, abrasions, punctures, burns, tenderness, swelling, and lacerations. If none of these are life-threats, they are ignored on scene and then begin immobilizing the patient on a long spine board.
The initial assessment, primary survey, and immobilization of the patient do not take more than ten minutes to achieve.
Steps:
- Mechanism of injury
- Evaluating patients with serious injuries or mechanisms of injury
- Evaluating patients with no significant mechanisms of injury
- Obtain Baseline Vital Signs Obtain SAMPLE History
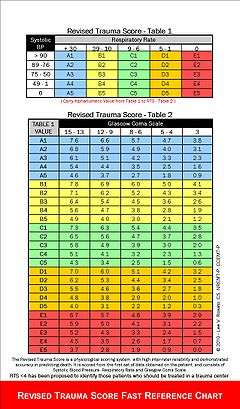
Determining a trauma score is also part of the trauma assessment. A patient's trauma can be evaluated by different scoring systems, but the most commonly used are the Glasgow Coma Scale and the Revised Trauma Score.
Ongoing assessment
The en route assessment starts when the patient is loaded in the ambulance. En route assessment begins with a repeat of the initial assessment and ensuring that the patient still has a patent airway, breathes or is being properly ventilated, and has a pulse. This is known as "taking (or checking) vitals."
Communications
EMS uses dedicated MED channels to communicate. EMS care providers should always inform other members of the system of their whereabouts, actions and status of a patient. This may include calling medical control or radioing ahead to the hospital to advise them that they should prepare to receive the patient, calling for air transport of a critical patient, or asking for law enforcement on the scene. Communication with other, perhaps more advanced levels of care providers can be an important part of a trauma assessment.
Documentation
With each patient interaction, even those in which transport is not provided, a Patient Care Report (PCR) should be completed. All important information must be included in the PCR, such as address, time, patient's chief complaint, any action taken by EMS personnel, and the patient's signs and symptoms. Every time a patient's vitals are assessed, they should be recorded in the dedicated vitals section of the PCR. Documentation is an especially important part of EMS work because legal issues are often encountered. With regard to reports, two helpful principles are:
1. If something is not recorded in the report, it is assumed to not have occurred.[1]
2. If the report is sloppy or otherwise inadequate, the medical care provided is assumed to be inadequate.[2]
It is not legally or ethically permissible to state assumptions as facts in an official report. Therefore, documentation of a traumatic injury should never include a description of the events leading up to the injury unless it is specifically stated that this is inferred based on evidence at the scene or that it is based on information provided by someone else. Further documentation is required when a patient refuses care or transport. A refusal of care form must be signed by the patient stating that they are refusing care despite having been fully informed of the risks inherent in their decision.[3]
References
- Sanders. Paramedic Textbook.
- Pollak, Andrew. Emergency Care and Transportation of the Sick and Injured.