Spinal precautions

Spinal precautions also known as spinal immobilization and spinal motion restriction are efforts to prevent movement of the spine in those with a risk of a spine injury.[1] This is done as an effort to prevent injury to the spinal cord.[1] It is estimated that 2% of people with blunt trauma will have a spine injury.[2]
Uses
Spinal immobilization was historically used routinely for people who had experienced physical trauma.[3] There is; however, little evidence for its routine use.[3] Long spine boards are often used in the prehospital environment as part of spinal immobilization.[4] Due to concerns of side effects the National Association of EMS Physicians and the American College of Surgeons recommend its use only in those at high risk.[4] This includes: those with blunt trauma who have a decreased level of consciousness, pain or tenderness in the spine, those with numbness or weakness believed to be due to a spinal injury and those with a significant trauma mechanism that are intoxicated or have other major injuries.[4] In those with a definite spinal cord injury immobilization is also recommended.[2]
Neck immobilization
There is little high quality evidence for immobilization of the neck before arrival at a hospital.[5][6] Using a hard cervical collar and attaching a person to an EMS stretcher may be sufficient in those who were walking after the accident or during long transports.[4] In those with penetrating neck or head trauma spinal immobilization may increase the risk of death.[5][7] If intubation is required the cervical collar should be removed and inline stabilization provided.[2]
Mid and low back immobilization
Spinal immobilization is not supported for penetrating trauma to back including that caused by gun shot wounds.[7]
Cervical spine clearance
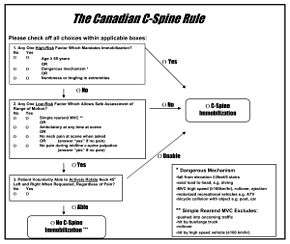
Paramedics are able to accurately determine who needs or does not need neck immobilization based on an algorithms.[2] There are two main algorithms, the Canadian C-spine rule and NEXUS. The Canadian C-spine rule appears to be better.[8] However, following either rule is reasonable.[9]
Adverse effects
Concern with use include: pain, agitation, and pressure ulcers.[4] A systematic review found cervical collar related skin ulcers from the devices in 7 to 38%.[10]
If a longboard is used, cushioning it is useful to decrease discomfort due to pressure.[2] A vacuum mattress and scoop board typically results in lower pressures.[2]
Mechanism of action
Studies with volunteers have found that using a hard collar, head stabilization with rolled up towels, and a long board decrease movement of the board.[2] What impact this has is unclear.[2]
References
- 1 2 Pollak, Andrew (1999). Refresher: Emergency Care and Transportation of the Sick and Injured. p. 302. ISBN 9780763709129.
- 1 2 3 4 5 6 7 8 Ahn, H; Singh, J; Nathens, A; MacDonald, RD; Travers, A; Tallon, J; Fehlings, MG; Yee, A (August 2011). "Pre-hospital care management of a potential spinal cord injured patient: a systematic review of the literature and evidence-based guidelines.". Journal of Neurotrauma. 28 (8): 1341–61. doi:10.1089/neu.2009.1168. PMC 3143405
 . PMID 20175667.
. PMID 20175667. - 1 2 Oteir, AO; Smith, K; Jennings, PA; Stoelwinder, JU (August 2014). "The prehospital management of suspected spinal cord injury: an update.". Prehospital and disaster medicine. 29 (4): 399–402. doi:10.1017/s1049023x14000752. PMID 25046238.
- 1 2 3 4 5 White CC, 4th; Domeier, RM; Millin, MG; Standards and Clinical Practice Committee, National Association of EMS, Physicians (Apr–Jun 2014). "EMS spinal precautions and the use of the long backboard - resource document to the position statement of the National Association of EMS Physicians and the American College of Surgeons Committee on Trauma.". Prehospital emergency care : official journal of the National Association of EMS Physicians and the National Association of State EMS Directors. 18 (2): 306–14. doi:10.3109/10903127.2014.884197. PMID 24559236.
- 1 2 Oteir, AO; Smith, K; Stoelwinder, JU; Middleton, J; Jennings, PA (12 January 2015). "Should suspected cervical spinal cord injury be immobilised?: A systematic review.". Injury. 46: 528–35. doi:10.1016/j.injury.2014.12.032. PMID 25624270.
- ↑ Sundstrøm, T; Asbjørnsen, H; Habiba, S; Sunde, GA; Wester, K (15 March 2014). "Prehospital use of cervical collars in trauma patients: a critical review.". Journal of Neurotrauma. 31 (6): 531–40. doi:10.1089/neu.2013.3094. PMID 23962031.
- 1 2 Stuke, LE; Pons, PT; Guy, JS; Chapleau, WP; Butler, FK; McSwain, NE (September 2011). "Prehospital spine immobilization for penetrating trauma--review and recommendations from the Prehospital Trauma Life Support Executive Committee.". The Journal of trauma. 71 (3): 763–9; discussion 769–70. doi:10.1097/ta.0b013e3182255cb9. PMID 21909006.
- ↑ Michaleff, ZA; Maher, CG; Verhagen, AP; Rebbeck, T; Lin, CW (6 November 2012). "Accuracy of the Canadian C-spine rule and NEXUS to screen for clinically important cervical spine injury in patients following blunt trauma: a systematic review.". Canadian Medical Association Journal. 184 (16): E867–76. doi:10.1503/cmaj.120675. PMID 23048086.
- ↑ Ackland, H; Cameron, P (April 2012). "Cervical spine - assessment following trauma.". Australian family physician. 41 (4): 196–201. PMID 22472679.
- ↑ Ham, W; Schoonhoven, L; Schuurmans, MJ; Leenen, LP (April 2014). "Pressure ulcers from spinal immobilization in trauma patients: a systematic review.". The journal of trauma and acute care surgery. 76 (4): 1131–41. doi:10.1097/ta.0000000000000153. PMID 24662882.