Vertical banded gastroplasty surgery
| Vertical banded gastroplasty surgery | |
|---|---|
| Intervention | |
| ICD-9-CM | 44.68 |
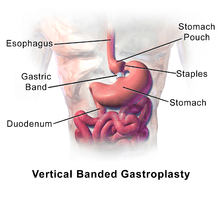
Vertical banded gastroplasty (VBG), also known as stomach stapling, is a restrictive operation for weight control. Both a band and staples are used to create a small stomach pouch. In the bottom of the pouch is an approximate one-centimeter hole through which the pouch contents can flow into the remainder of the stomach and thence onto the remainder of the gastrointestinal tract.
Stomach stapling is a restrictive technique for managing obesity. The pouch limits the amount of food a patient can eat at one time and slows passage of the food. Stomach stapling is more effective when combined with a malabsorptive technique, in which part of the digestive tract is bypassed, reducing the absorption of calories and nutrients. Combined restrictive and malabsorptive techniques are called gastric bypass techniques, of which Roux-en-Y gastric bypass surgery (RGB) is the most common. In this technique, staples are used to form a pouch that is connected to the small intestine, bypassing the lower stomach, the duodenum, and the first portion of the jejunum.
This type of weight loss surgery is losing favor as more doctors begin using the adjustable gastric band. The newer adjustable band does not require cutting into the stomach and does not use any staple lines, thus making it a much safer alternative.
Advantages and disadvantages
Advantages
- No dumping syndrome.
- No nutritional deficiencies/malabsorption.
Disadvantages
- Needs strict patient compliance to diet.
- High fibre foods and foods with a more dense, natural consistency can become very difficult to eat, while highly refined foods cause little discomfort. Most people who regain any weight lost after surgery do so because of choosing "healthier" foods that are harder to digest, while "junk" foods pass easily.
- VBG is in no way a magic bullet or pill. It must be emphasized that lifestyle changes, e.g., diet and exercise, are absolutely imperative for weight loss to occur and be maintained. Realistic expectations are imperative.
- Reversal of a VBG requires a much more complex and intensive surgical process than getting the VBG. When removal of a polyurethane band is involved (polyurethane was predominantly used in the 1980s and 90s), it likely has built substantial scar tissue that must also be removed, depending on how long ago the VBG took place. Removal of the staples involves stitching the previously separated parts of the stomach back together. For these reasons, a reversal should only be considered if there are serious medical complications.
- Vomiting and severe discomfort if food is not properly chewed or if food is eaten too quickly.
- Not adjustable (as with the adjustable gastric band, aka "lap band")).
Alternatives
- Duodenal switch surgery
- Vertical sleeve gastrectomy
- Roux-en-Y gastric bypass
- Selective vagotomy (snipping the vagus nerve, effectively stopping hunger sensations).
- Mini gastric bypass
Long term
Although restrictive operations lead to weight loss in almost all patients, they are less successful than malabsorptive operations in achieving substantial, long-term weight loss. About 30% of those who undergo VBG achieve normal weight, and about 80% achieve some degree of weight loss. Most studies have suggested that 10 years after surgery, only 10% of patients maintain a minimum weight loss of at least 50% of their total excess weight at the time of their initial surgery. Some patients regain weight. Others are unable to adjust their eating habits and fail to lose the desired weight. Successful results depend on the patient’s willingness to adopt a long-term plan of healthy eating and regular physical activity. According to an episode of Oprah Winfrey that aired on October 24, 2006, 30% of people who undergo weight loss surgery such as VBG or gastric bypass suffer from addiction transference, which is transferring the previous addiction to food with a new addiction to alcoholism. The show stressed the importance of examining the root causes of addiction in order to avoid the phenomenon.
History
Vertical banded gastroplasty was developed in 1980 by Dr. Edward E. Mason at the University of Iowa. Dr. Mason also developed the original gastric bypass for weight reduction in 1966 and is known for his pioneering work as the "father of obesity surgery".