Veress needle
A Veress needle is a spring-loaded needle used to create pneumoperitoneum for laparoscopic surgery. Of the three general approaches to laparoscopic access, the Veress needle technique is the oldest and most traditional.
History
The tool was first developed in 1932 by Janos Veress, a Hungarian internist working with tuberculosis patients. At the time, one of the mainstays of treatment was to collapse an infected lung and allow lesions to heal.[1] The needle was introduced as a safer technique to give patients such pneumothoraces. It was not until 1938, when he published his invention in the German literature, that the needle became more broadly known outside of Hungary.[2]
Raoul Palmer introduced the use of the Veress needle in laparoscopy to establish a pneumoperitoneum.[3]
Description
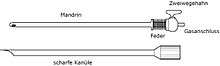
Modern needles are 12 to 15 cm long, with an external diameter of 2 mm. The outer cannula consists of a beveled needle point for cutting through tissues of the abdominal wall. A spring-loaded, inner stylet is positioned within the outer cannula. This inner stylet has a dull tip to protect any viscera from injury by the sharp, outer cannula. Direct pressure on the tip—as when penetrating through tissue—pushes the dull stylet into the shaft of the outer cannula. When the tip of the needle enters a space such as the peritoneal cavity, the dull, inner stylet springs forward. Carbon dioxide is then passed through the Veress needle to inflate the space, creating a pneumoperitoneum.[4]
Use
In a large survey of 155,987 gynecologic procedures and 17,216 general surgery procedures, the Veress needle technique was used in 78% of them. Gynecologists (81%) used the tool more often than general surgeons (48%) who are far more likely to use the open access technique.[5]
Iatrogenics
It has been pointed out that the use of Veress needle to achieve pneumoperitoneum is not as safe as other methods. Between the complications associated to this instrument it can be found:
- Injury to hollow viscous
- Bleeding
- Failure to achieve penumoperitoneum
- Prepneumoperitoneum
- Biloma due to liver puncture.[6]
- Vascular injury
See also
References
- ↑ Wolfart W (1990). "Surgical treatment of tuberculosis and its modifications—collapse therapy and resection treatment and their present-day sequelae". Offentl Gesundheitswes. 52 (8–9): 506–11. PMID 2146567.
- ↑ Veres J (1938) Neues instrument zur ausfuhrung von brust-oder bauchpunktionen und pneumothoraxbehandlung. Deut Med Wochenschr 64: 1480–1481
- ↑ Palmer, R (1947). "Instrumentation et technique de la coelioscopie gynecologique.". Gynecol Obstet (Paris) 1947;46:420–431. 46: 420–31. PMID 18917806.
- ↑ Gould JC, Philip A. Principles and Techniques of Abdominal Access and Physiology of Pneumoperitoneum. In: Ashley SW. Scientific American Surgery. Decker Intellectual Properties; 2011.
- ↑ Molloy D, Kaloo PD, Cooper M, et al. Laparoscopic entry: a literature review and analysis of techniques and complications of primary port entry. Aust N Z J Obstet Gynaecol 2002;42:246-53.
- ↑ Segura-Sampedro JJ, Cañete-Gómez J, Reguera-Rosal J, Padillo-Ruiz FJ, Ramírez-Plaza CP (Jul 2015). "Unnoticed biloma due to liver puncture after Veress needle insertion". Ann Med Surg (Lond). 4 (3): 238–239,. doi:10.1016/j.amsu.2015.07.016. PMC 4624565
 . PMID 26587233.
. PMID 26587233.