Carboplatin
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | /ˈkɑːrboʊˌplætən/ |
| Trade names | Paraplatin |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a695017 |
| Pregnancy category |
|
| Routes of administration | Intravenous |
| ATC code | L01XA02 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | complete |
| Protein binding | Very low |
| Biological half-life | 1.1-2 hours |
| Excretion | renal |
| Identifiers | |
| |
| CAS Number |
41575-94-4 |
| PubChem (CID) | 498142 |
| DrugBank |
DB00958 |
| ChemSpider |
8514637 |
| UNII |
BG3F62OND5 |
| KEGG |
D01363 |
| ChEBI |
CHEBI:31355 |
| ChEMBL |
CHEMBL288376 |
| ECHA InfoCard | 100.050.388 |
| Chemical and physical data | |
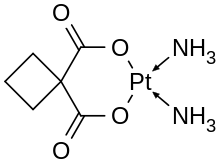
| Formula | C6H12N2O4Pt |
| Molar mass | 371.249 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
| | |
Carboplatin, sold under the trade name Paraplatin among others, is a chemotherapy drug used against some forms of cancer (mainly ovarian carcinoma, lung, head and neck cancers as well as endometrial, esophageal, bladder, breast and cervical; central nervous system or germ cell tumors; osteogenic sarcoma, and as preparation for a stem cell or bone marrow transplant).[1][2] It was introduced in the late 1980s and has since gained popularity in clinical treatment due to its vastly reduced side effects compared to its parent compound cisplatin. Cisplatin and carboplatin belong to the group of platinum-based antineoplastic agents, and interact with DNA to interfere with DNA repair.
It is on the World Health Organization's List of Essential Medicines, a list of the most important medications needed in a basic health system.[3]
Side-effects
Relative to cisplatin, the greatest benefit of carboplatin is its reduced side effects, particularly the elimination of nephrotoxic effects. Nausea and vomiting are less severe and more easily controlled.
The main drawback of carboplatin is its myelosuppressive effect. This causes the blood cell and platelet output of bone marrow in the body to decrease quite dramatically, sometimes as low as 10% of its usual production levels. The nadir of this myelosuppression usually occurs 21–28 days after the first treatment, after which the blood cell and platelet levels in the blood begin to stabilize, often coming close to its pre-carboplatin levels. This decrease in white blood cells (neutropenia) can cause complications, and is sometimes treated with drugs like filgrastim. The most notable complication of neutropenia is increased probability of infection by opportunistic organisms, which necessitates hospital readmission and treatment with antibiotics.
Carboplatin is less potent than cisplatin; depending on the strain of cancer, carboplatin may only be 1/8 to 1/45 as effective. The clinical standard of dosage of carboplatin is usually a 4:1 ratio compared to cisplatin; that is, for a dose that usually requires a particular dose of cisplatin, four times as much carboplatin is needed to achieve the same effectiveness. The stable property of carboplatin is a mixed blessing: once uptake of the drug occurs, its retention half-life is considerably longer than cisplatin, but it is also this inertness that causes carboplatin to go right through the human body, and up to 90% of the carboplatin given can be recovered in urine.
Chemistry
In terms of its structure, carboplatin differs from cisplatin in that it has a bidentate dicarboxylate (the ligand is CycloButane DiCarboxylic Acid, CBDCA) in place of the two chloride ligand, which are the leaving groups in cisplatin. For this reason, "CBDCA" is sometimes used in the medical literature as an abbreviation referring to carboplatin. Carboplatin exhibits lower reactivity and slower DNA binding kinetics, although it forms the same reaction products in vitro at equivalent doses with cisplatin. Unlike cisplatin, carboplatin may be susceptible to alternative mechanisms. Some results show that cisplatin and carboplatin cause different morphological changes in MCF-7 cell lines while exerting their cytotoxic behaviour.[4] The diminished reactivity limits protein-carboplatin complexes, which are excreted. The lower excretion rate of carboplatin means that more is retained in the body, and hence its effects are longer lasting (a retention half-life of 30 hours for carboplatin, compared to 1.5-3.6 hours in the case of cisplatin).
Mechanism of action
Two theories exist to explain the molecular mechanism of action of carboplatin with DNA:
- Aquation, or the like-cisplatin hypothesis.
- Activation, or the unlike-cisplatin hypothesis.
The former is more accepted owing to the similarity of the leaving groups with its predecessor cisplatin, while the latter hypothesis envisages a biological activation mechanism to release the active Pt2+ species.
Dose
Calvert's formula is used to calculate the dose of carboplatin. It takes under consideration the creatinine clearance and the desired area under curve.[5]
History
Carboplatin was discovered at Michigan State University,[6] and developed at the Institute of Cancer Research in London. Bristol-Myers Squibb gained Food and Drug Administration (FDA) approval for carboplatin, under the brand name Paraplatin, in March 1989. Starting in October 2004, generic versions of the drug became available.
Current events
A recent study in mutant mice suggests that in the subset of women with breast cancer due to BRCA1 and BRCA2 genes (these cause a variety of familial breast cancer) carboplatin may be as much as 20 times more effective than the usual breast cancer treatments.[7] However, similar data in humans has not yet been shown.
Carboplatin has also been used for adjuvant therapy of stage 1 seminomatous testicular cancer. Research has indicated that it is not less effective than adjuvant radiotherapy for this treatment, while having fewer side effects.[8] This has led to carboplatin based adjuvant therapy being generally preferred over adjuvant radiotherapy in clinical practice.[9]
See also
References
- ↑ Wheate NJ, Walker S, Craig GE, Oun R (September 2010). "The status of platinum anticancer drugs in the clinic and in clinical trials". Dalton Transactions. 39 (35): 8113–27. doi:10.1039/C0DT00292E. PMID 20593091.
- ↑ Apps, M. G.; Choi, E. H. Y.; Wheate, N. J. (2015). "The state-of-play and future of platinum drugs". Endocrine-related Cancer. 22 (4): 219–233. doi:10.1530/ERC-15-0237. PMID 26113607.
- ↑ "WHO Model List of EssentialMedicines" (PDF). World Health Organization. October 2013. Retrieved 22 April 2014.
- ↑ Natarajan G, Malathi R, Holler E (November 1999). "Increased DNA-binding activity of cis-1,1-cyclobutanedicarboxylatodiammineplatinum(II) (carboplatin) in the presence of nucleophiles and human breast cancer MCF-7 cell cytoplasmic extracts: activation theory revisited". Biochemical Pharmacology. 58 (10): 1625–29. doi:10.1016/S0006-2952(99)00250-6. PMID 10535754.
- ↑ http://www.mskcc.org/cancer-care/clinical-update/new-guidelines-carboplatin-dosing
- ↑ "Discovery to Market: Fact Sheet".
- ↑ Henderson, Mark (May 1, 2006). "Lung cancer drug may fight breast tumour in women". Times Online.
- ↑ Oliver RT, Mason MD, Mead GM, von der Maase H, Rustin GJ, Joffe JK, de Wit R, Aass N, Graham JD, Coleman R, Kirk SJ, Stenning SP (2005). "Radiotherapy versus single-dose carboplatin in adjuvant treatment of stage I seminoma: a randomised trial". Lancet. 366 (9482): 293–300. doi:10.1016/S0140-6736(05)66984-X. PMID 16039331.
- ↑ Toner GC (2015). "Testicular cancer: Optimal management of stage I seminoma in 2015". Nat Rev Urol. 12 (5): 249–51. doi:10.1038/nrurol.2015.85. PMID 25896179.
Additional references
- Natarajan G, Malathi R, Holler E (November 1999). "Increased DNA-binding activity of cis-1,1-cyclobutanedicarboxylatodiammineplatinum(II) (carboplatin) in the presence of nucleophiles and human breast cancer MCF-7 cell cytoplasmic extracts: activation theory revisited". Biochem. Pharmacol. 58 (10): 1625–9. doi:10.1016/S0006-2952(99)00250-6. PMID 10535754.
- Knox RJ, Friedlos F, Lydall DA, Roberts JJ (April 1986). "Mechanism of cytotoxicity of anticancer platinum drugs: evidence that cis-diamminedichloroplatinum(II) and cis-diammine-(1,1-cyclobutanedicarboxylato)platinum(II) differ only in the kinetics of their interaction with DNA". Cancer Res. 46 (4 Pt 2): 1972–9. PMID 3512077.
- Canetta R, Rozencweig M, Carter SK (September 1985). "Carboplatin: the clinical spectrum to date". Cancer Treat. Rev. 12 (Suppl A): 125–36. doi:10.1016/0305-7372(85)90027-1. PMID 3002623.
- Overbeck TL, Knight JM, Beck DJ (April 1996). "A comparison of the genotoxic effects of carboplatin and cisplatin in Escherichia coli". Mutat. Res. 362 (3): 249–59. doi:10.1016/0921-8777(95)00056-9. PMID 8637503.
- Schnurr B, Gust R (August 2002). "Investigations on the decomposition of carboplatin in infusion solutions". Mikrochimica Acta. 140 (1–2): 69–76. doi:10.1007/s006040200070.
- Yang XL, Wang AH (September 1999). "Structural studies of atom-specific anticancer drugs acting on DNA". Pharmacol. Ther. 83 (3): 181–215. doi:10.1016/S0163-7258(99)00020-0. PMID 10576292.
- Travis LB, Holowaty EJ, Bergfeldt K, et al. (February 1999). "Risk of leukemia after platinum-based chemotherapy for ovarian cancer". N. Engl. J. Med. 340 (5): 351–7. doi:10.1056/NEJM199902043400504. PMID 9929525.