Cardiac tamponade
| Cardiac tamponade | |
|---|---|
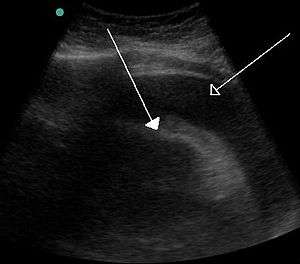 | |
| A very large pericardial effusion resulting in tamponade as a result of bleeding from cancer as seen on ultrasound. closed arrow: the heart, open arrow: the effusion | |
| Classification and external resources | |
| Specialty | Cardiac surgery |
| ICD-10 | I31.9 |
| ICD-9-CM | 423.3 |
| MedlinePlus | 000194 |
| eMedicine | med/283 emerg/412 |
| Patient UK | Cardiac tamponade |
| MeSH | D002305 |
Cardiac tamponade, also known as pericardial tamponade, is when fluid in the pericardium (the sac around the heart) builds up and results in compression of the heart.[1] Onset may be rapid or more gradual.[1] Symptoms typically include those of cardiogenic shock including shortness of breath, weakness, lightheadedness, and cough. Other symptoms may relate to the underlying cause.[2]
Common causes include cancer, kidney failure, chest trauma, and pericarditis.[1] Other causes include connective tissue diseases, hypothyroidism, aortic rupture, and following cardiac surgery.[3] In Africa, tuberculosis is a relatively common cause.[2]
Diagnosis may be suspected based on low blood pressure, jugular venous distension, pericardial rub, or quiet heart sounds.[1][2] The diagnosis may be further supported by specific electrocardiogram (ECG) changes, chest X-ray, or an ultrasound of the heart.[1] If fluid increases slowly the pericardial sac can expand to contain more than 2 liters; however, if the increase is rapid as little as 200 mL can result in tamponade.[1]
When tamponade results in symptoms, drainage is necessary.[4] This can be done by pericardiocentesis, surgery to create a pericardial window, or a pericardiectomy.[1] Drainage may also be necessary to rule out infection or cancer.[4] Other treatments may include the use of dobutamine or in those with low blood volume, intravenous fluids.[2] Those with few symptoms and no worrisome features can often be closely followed.[1] The frequency of tamponade is unclear.[5] One estimate from the United States places it at 2 per 10,000 per year.[6]
Signs and symptoms
Onset may be rapid or more gradual.[1] Symptoms typically include those of cardiogenic shock including shortness of breath, weakness, lightheadedness, and cough.[2] Other symptoms may relate to the underlying cause.[2]
Causes
Cardiac tamponade is caused by a large or uncontrolled pericardial effusion, i.e. the buildup of fluid inside the pericardium.[7] This commonly occurs as a result of chest trauma (both blunt and penetrating),[8] but can also be caused by myocardial rupture, cancer, uremia, pericarditis, or cardiac surgery,[7] and rarely occurs during retrograde aortic dissection,[9] or while the person is taking anticoagulant therapy.[10] The effusion can occur rapidly (as in the case of trauma or myocardial rupture), or over a more gradual period of time (as in cancer). The fluid involved is often blood, but pus is also found in some circumstances.[7]
Causes of increased pericardial effusion include hypothyroidism, physical trauma (either penetrating trauma involving the pericardium or blunt chest trauma), pericarditis (inflammation of the pericardium), iatrogenic trauma (during an invasive procedure), and myocardial rupture.
Surgery
One of the most common settings for cardiac tamponade is in the first 24 to 48 hours after heart surgery. After heart surgery, chest tubes are placed to drain blood. These chest tubes, however, are prone to clot formation. When a chest tube becomes occluded or clogged, the blood that should be drained can accumulate around the heart, leading to tamponade.
Pathophysiology
The outer layer of the heart is made of fibrous tissue[11] which does not easily stretch, so once fluid begins to enter the pericardial space, pressure starts to increase.[7]
If fluid continues to accumulate, each successive diastolic period leads to less blood entering the ventricles. Eventually, increasing pressure on the heart forces the septum to bend in towards the left ventricle, leading to a decrease in stroke volume.[7] This causes the development of obstructive shock, which if left untreated may lead to cardiac arrest (often presenting as pulseless electrical activity).
Diagnosis
Initial diagnosis can be challenging, as there are a number of differential diagnoses, including tension pneumothorax,[8] and acute heart failure. In a trauma patient presenting with PEA (pulseless electrical activity) in the absence of hypovolemia and tension pneumothorax, the most likely diagnosis is cardiac tamponade.[12]
Signs of classical cardiac tamponade include three signs, known as Beck's triad. Low blood pressure occurs because of decreased stroke volume, jugular-venous distension due to impaired venous return to the heart, and muffled heart sounds due to fluid buildup inside the pericardium.[13]
Other signs of tamponade include pulsus paradoxus (a drop of at least 10 mmHg in arterial blood pressure with inspiration),[7] and ST segment changes on the electrocardiogram,[13] which may also show low voltage QRS complexes,[10] as well as general signs and symptoms of shock (such as fast heart rate, shortness of breath and decreasing level of consciousness). However, some of these signs may not be present in certain cases. A fast heart rate, although expected, may be absent in people with uremia and hypothyroidism.[2]
In addition to the diagnostic complications afforded by the wide-ranging differential diagnosis for chest pain, diagnosis can be additionally complicated by the fact that patients will often be weak or faint at presentation. For instance, a fast rate of breathing and difficulty breathing on exertion that progresses to air hunger at rest can be a key diagnostic symptom, but it may not be possible to obtain such information from patients who are unconscious or who have convulsions at presentation.[2]
Tamponade can often be diagnosed radiographically. Echocardiography, which is the diagnostic test of choice, often demonstrates an enlarged pericardium or collapsed ventricles. A large cardiac tamponade will show as an enlarged globular-shaped heart on chest x-ray. During inspiration, the negative pressure in the thoracic cavity will cause increased pressure into the right ventricle. This increased pressure in the right ventricle will cause the interventricular septum to bulge towards the left ventricle, leading to decreased filling of the left ventricle. At the same time, right ventricle volume is markedly diminished and sometimes it can collapse.[10]
Treatment
Pre-hospital care
Initial treatment given will usually be supportive in nature, for example administration of oxygen, and monitoring. There is little care that can be provided pre-hospital other than general treatment for shock. Some teams have performed an emergency thoracotomy to release clotting in the pericardium caused by a penetrating chest injury.
Prompt diagnosis and treatment is the key to survival with tamponade. Some pre-hospital providers will have facilities to provide pericardiocentesis, which can be life-saving. If the patient has already suffered a cardiac arrest, pericardiocentesis alone cannot ensure survival, and so rapid evacuation to a hospital is usually the more appropriate course of action.
Hospital management
Initial management in hospital is by pericardiocentesis.[8] This involves the insertion of a needle through the skin and into the pericardium and aspirating fluid under ultrasound guidance preferably. This can be done laterally through the intercostal spaces, usually the fifth, or as a subxiphoid approach.[14][15] A left parasternal approach begins 3 to 5 cm left of the sternum to avoid the left internal mammary artery, in the 5th intercostal space.[16] Often, a cannula is left in place during resuscitation following initial drainage so that the procedure can be performed again if the need arises. If facilities are available, an emergency pericardial window may be performed instead,[8] during which the pericardium is cut open to allow fluid to drain. Following stabilization of the patient, surgery is provided to seal the source of the bleed and mend the pericardium.
In heart surgery patients post op, the nurses monitor the amount of chest tube drainage. If the drainage volume drops off, and the blood pressure goes down, this can suggest tamponade due to chest tube clogging. In that case, the patient is taken back to the operating room for an emergency reoperation.
If aggressive treatment is offered immediately and no complications arise (shock, AMI or arrhythmia, heart failure, aneurysm, carditis, embolism, or rupture), or they are dealt with quickly and fully contained, then adequate survival is still a distinct possibility.
Epidemiology
The frequency of tamponade is unclear.[5] One estimate from the United States places it at 2 per 10,000 per year.[6] It is estimated to occur in 2% of those with stab or gunshot wounds to the chest.[17]
References
- 1 2 3 4 5 6 7 8 9 Richardson, L (November 2014). "Cardiac tamponade.". JAAPA : official journal of the American Academy of Physician Assistants. 27 (11): 50–1. PMID 25343435.
- 1 2 3 4 5 6 7 8 Spodick, DH (Aug 14, 2003). "Acute cardiac tamponade.". The New England Journal of Medicine. 349 (7): 684–90. doi:10.1056/NEJMra022643. PMID 12917306.
- ↑ Schiavone, WA (February 2013). "Cardiac tamponade: 12 pearls in diagnosis and management.". Cleveland Clinic journal of medicine. 80 (2): 109–16. PMID 23376916.
- 1 2 Sagristà-Sauleda, J; Mercé, AS; Soler-Soler, J (26 May 2011). "Diagnosis and management of pericardial effusion.". World journal of cardiology. 3 (5): 135–43. PMID 21666814.
- 1 2 Bodson, L; Bouferrache, K; Vieillard-Baron, A (October 2011). "Cardiac tamponade.". Current opinion in critical care. 17 (5): 416–24. PMID 21716107.
- 1 2 Kahan, Scott (2008). In a Page: Medicine. Lippincott Williams & Wilkins. p. 20. ISBN 9780781770354.
- 1 2 3 4 5 6 Porth, Carol; Carol Mattson Porth (2005). Pathophysiology: concepts of altered health states (7th ed.). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-4988-3.
- 1 2 3 4 Gwinnutt CL, Driscoll PA (2003). Trauma Resuscitation: The Team Approach (2nd ed.). Oxford: BIOS. ISBN 1-85996-009-X.
- ↑ Isselbacher EM, Cigarroa JE, Eagle KA (Nov 1994). "Cardiac tamponade complicating proximal (retrograde) aortic dissection. Is pericardiocentesis harmful?". Circulation. 90 (5): 2375–8. doi:10.1161/01.CIR.90.5.2375. PMID 7955196.
- 1 2 3 Longmore, J. M.; Murray Longmore; Wilkinson, Ian; Supraj R. Rajagopalan (2004). Oxford handbook of clinical medicine (6th ed.). Oxford [Oxfordshire]: Oxford University Press. ISBN 0-19-852558-3.
- ↑ Patton KT, Thibodeau GA (2003). Anatomy & physiology (5th ed.). St. Louis: Mosby. ISBN 0-323-01628-6.
- ↑ American College of Surgeons Committee on Trauma (2007). Advanced Trauma Life Support for Doctors, 7th Edition. Chicago: American College of Surgeons
- 1 2 Holt L, Dolan B (2000). Accident and emergency: theory into practice. London: Baillière Tindall. ISBN 0-7020-2239-X.
- ↑ Shlamovitz, Gil (4 August 2011). "Pericardiocentesis". Medscape. Retrieved 16 August 2011.
- ↑ Yarlagadda, Chakri (11 August 2011). "Cardiac Tamponade Treatment & Management". Medscape. Retrieved 16 August 2011.
- ↑ Synovitz C.K., Brown E.J. (2011). Chapter 37. Pericardiocentesis. In Tintinalli J.E., Stapczynski J, Ma O, Cline D.M., Cydulka R.K., Meckler G.D., T (Eds), Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e. Retrieved September 19, 2014 from http://accessmedicine.mhmedical.com/content.aspx?bookid=348&Sectionid=40381499.
- ↑ Marx, John; Walls, Ron; Hockberger, Robert (2013). Rosen's Emergency Medicine - Concepts and Clinical Practice. Elsevier Health Sciences. p. 448. ISBN 1455749877.