Trichostrongylus
| Trichostrongylus | |
|---|---|
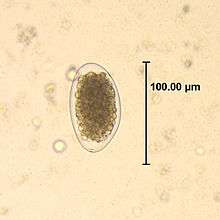 | |
| Egg of Trichostrongylus sp. | |
| Scientific classification | |
| Kingdom: | Animalia |
| Phylum: | Nematoda |
| Class: | Chromadorea |
| Order: | Rhabditida |
| Family: | Trichostrongylidae |
| Genus: | Trichostrongylus |
| Species: | Trichostrongylus affinis |
Trichostrongylus species are nematodes (round worms), which are ubiquitous among herbivores worldwide, including cattle, sheep, donkeys, goats, deer, and rabbits.[1][2][3] At least 10 Trichostrongylus species have been associated with human infections.[1] Infections occur via ingestion of infective larvae from contaminated vegetables or water.[1][3] Epidemiological studies indicate a worldwide distribution of Trichostrongylus infections in humans, with the highest prevalence rates observed in individuals from regions with poor sanitary conditions, in rural areas, or who are farmers / herders.[4][5] Human infections are most prevalent in the Middle East and Asia,[3] with a worldwide estimated prevalence of 5.5 million people.[1]
Clinical presentation
The majority of human infections are asymptomatic or associated with mild symptoms. Symptomatic individuals may experience abdominal pain, nausea, diarrhea, flatulence, dizziness, generalized fatigue, and malaise.[1][2][3] Eosinophilia is frequently observed.[1][2][3] Infections with a heavy worm burden can lead to anemia, cholecystitis, and emaciation.[1][3]
Diagnosis
The adult worms live in the small intestine. The diagnosis is based on the observation of eggs in the stool. The eggs are 85–115 um, oval, elongated, and pointed at one or both ends.[3] Trichostrongylus eggs must be differentiated from hookworm eggs, which are smaller and do not have pointed ends.[1][3]
Prevention and treatment
Since the use of herbivore manure as fertilizer is a common practice preceding infection, thorough cleaning and cooking of vegetables is required for prevention of infection.[1][3] Treatment with pyrantel pamoate is recommended.[6] Alternative agents include mebendazole and albendazole.[6] Successful treatment with ivermectin has also been reported.[2]
References
- 1 2 3 4 5 6 7 8 9 Garcia LS, editor. Diagnostic Medical Parasitology. 5 ed. Washington, DC: ASM Press; 2007.
- 1 2 3 4 Ralph A, O'Sullivan M, Sangster N, Walker J. Abdominal pain and eosinophilia in suburban goat keepers - Trichostrongylosis. Med J Aust. 2006;184(9):467-9.
- 1 2 3 4 5 6 7 8 9 Strickland GT, editor. Hunter's Tropical Medicine and Emerging Infectious Diseases. 8 ed. Philadelphia, PA: WB Saunders Company; 2000.
- ↑ Adams VJ, Markus MB, Adams JF, Jordaan E, Curtis B, Dhansay MA, et al. Paradoxical helminthiasis and giardiasis in Cape Town, South Africa: epidemiology and control. Afr Health Sci. 2005 Sep;5(3):276-80.
- ↑ el-Shazly AM, el-Nahas HA, Soliman M, Sultan DM, Abedl Tawab AH, Morsy TA. The reflection of control programs of parasitic diseases upon gastrointestinal helminthiasis in Dakahlia Governorate, Egypt. J Egypt Soc Parasitol. 2006 Aug;36(2):467-80.
- 1 2 Drugs for parasitic infections. The Med Lett. 2007;5(Suppl):1-15.